Yuan-Yuan Cheng, Ph.D.
International Ph.D. Program in Cell Therapy and Regenerative Medicine,
College of Medicine, Taipei Medical University, Taiwan
Abstract
Background
Heart disease remains the second leading cause of death worldwide. Currently, heart transplantation is considered the only definitive treatment for severe heart failure due to the poor heart regeneration after injury. Adult cardiomyocytes lose their proliferative ability after birth, leading to insufficient compensation for the infarcted myocardium. Therefore, to complete heart regeneration continues to present a major challenge in cardiac therapy.
Findings
Following the discovery of induced pluripotent stem cell (iPSC) technology, iPSC-derived cardiomyocytes (iPSC-CMs) have been generally considered as a promising cell source for cardiac regeneration. However, direct cell injection is associated with poor cell survival and limited engraftment efficiency. To overcome these limitations, cell sheet technology was developed and subsequently combined with iPSC-CMs to provide direct contractile contribution and partial myocardial replacement. ReHeart/RiHeart, which integrates cell sheet engineering with iPSC technology, has become the first conditionally approved iPSC-derived cardiac regenerative therapy worldwide. Nevertheless, to achieve true long-term remuscularization of the injured myocardium remains a major challenge.
Conclusion
ReHeart/RiHeart represents a major step forward in translational cardiac regenerative medicine and provides an important foundation for the future development of clinically effective heart regenerative therapies.
Keywords: iPSC, ReHeart/RiHeart, Cell sheet, Heart regeneration
Introduction
Heart regeneration has long been considered impossible because cardiac myocytes lose their proliferative capacity after cardiac injury. To date, heart transplantation remains the gold-standard therapy for end-stage heart failure; however, the severe shortage of donor hearts continues to limit its clinical application1. Recent advances in induced pluripotent stem cell
(iPSC) technology have provided new hope for heart regeneration1,2. Notably, the first conditionally approved clinical application utilizes iPSC-derived cardiomyocyte (iPSC-CM) sheets, known as ReHeart/RiHeart, developed by Osaka University in collaboration with Cuorips3,4. This achievement represents a major step forward in the field of cardiac regeneration.
In this review, I first introduce the major milestones in the development of cell sheet technology for cardiac repair after injury and further summarize the different cell types that have been applied to generate cardiac cell sheets. Finally, ReHeart/RiHeart is highlighted as a representative example to illustrate both the significant advances achieved and the remaining challenges that still need to be overcome in clinical cardiac regeneration.
FINDINGS/MAIN TEXT
The history of cell sheet technology for heart regeneration
Cell sheet is a tissue engineering technique that utilizes a contiguous layer of cells with preserved extracellular matrix (ECM)5. It can be harvested and transplanted without enzyme digestion. The development of cell sheet technology can be traced back to the early 2000s, when researchers discovered that extremely low cell retention after direct cell injection6. Dr. Teruo Okano’s group developed a temperature-responsive culture dish to generate intact cell sheets7. When the temperature is reduced to 20℃, the culture surface becomes hydrophilic to enable the cells spontaneously detach as an intact sheet rather than as dissociated single cells. Through this harvesting method, the ECM, cell-cell junction, and surface proteins are largely preserved to generate tissue-like cell sheets. In 2002, Drs. Shimizu and Okano group published the first cardiac cell sheet generated from primary neonatal rat CMs cultured on temperature-responsive culture dishes8. Importantly, these layered cell sheets exhibited synchronous contraction and electrical coupling between layers8. However, the first clinical application of cell sheet technology in cardiac repair utilized skeletal myoblast sheets, pioneered by Dr. Yoshiki Sawa’s group in Japan in 20109,10. Autologous skeletal myoblast sheet transplantation demonstrated improved cardiac function and symptoms in patients with severe heart failure, including reduced hospitalization rates. Nevertheless, the limited electrical integration and non-CM nature of skeletal myoblasts remained major concerns. To overcome these limitations, mesenchymal stem cell (MSC)-based and iPSC-derived cardiac cell sheets were subsequently developed11,12. In 2012, human iPSC-engineered cardiac tissue sheets were first generated and transplanted into infarcted rat hearts, resulting in improved cardiac function12. After that, the clinical-grade production and translational application of cardiac patches rapidly advanced, ultimately leading to the first conditional approval of an iPSC-derived cardiac regeneration therapy, ReHeart/RiHeart3,4. Figure 1 summarizes the major milestones in the development of cell sheet technology for cardiac regeneration.
Cell sources to generate cell sheets for heart regeneration
The first cell source used for generating cell sheets for heart regeneration was skeletal myoblasts. Autologous transplantation, ischemic resistance, and high proliferative capacity
made skeletal myoblasts an attractive candidate for early cardiac cell sheet studies10,13 (Figure 2). Initial studies demonstrated that skeletal myoblast-derived cell sheets improved heart function after myocardial infarction (MI) by enhancing systolic function, reducing left ventricular wall thickness, and promoting neovascularization10,13. Furthermore, combining the omentum with skeletal myoblast-derived cell sheets significantly enhanced cell engraftment within the infarct area of the injured hearts14,15. Even more encouragingly, obvious functional recovery was observed in patients suffering from dilated or ischemic cardiomyopathy14,15. However, the limited CM differentiation potential and poor electrical integration with resident CMs restricted the clinical application of skeletal myoblast-derived cell sheets for cardiac regeneration13,16.
Due to their ease of isolation and autologous availability, MSC subsequently emerged as another promising cell source for cardiac cell sheet generation11. MSCs can be isolated from bone marrow, adipose tissue, and placenta, and their therapeutic benefits are largely attributed to paracrine signaling that supports vascularization and cardiac protection after injury17. MSC-derived cell sheets were reported to attenuate adverse cardiac remodeling and reduce fibrosis in mouse and rat MI models11,18. However, because MSCs exhibited limited capacity to differentiate into functional CMs19,20, their practical application in true myocardial regeneration remains constrained.
Through the discovery of iPSCs by Dr. Shinya Yamanaka in 20062, a promising cell source for cardiac regeneration became available. Due to their pluripotency and self-renewal capacity, iPSCs exhibit strong potential to differentiate into CMs and therefore emerged as an ideal cell source for generating cardiac cell sheets21. In 2012, human iPSC-CM sheets were successfully generated with high differentiation efficiency by Drs. Masumoto and Sawa, and colleagues at Osaka University12. Importantly, transplantation of these iPSC-CM sheets improved cardiac function by enhancing neovascularization, attenuating LV remodeling, and promoting cardiomyogenesis in rat MI models12. Subsequently, in 2013, human iPSC-CM sheets combined with an omental flap were further shown to enhance graft survival and engraftment within infarcted regions, which resulted in additional improvement of cardiac function in porcine MI models22. Building upon these findings, a clinical-grade allogeneic cardiac patch platform, ReHeart/RiHeart, was developed by Osaka University in collaboration with Cuorips3,4. This platform successfully advanced to clinical trials and ultimately became the first conditional approved iPSC-derived cardiac regenerative therapy worldwide.
Advantages and limitation of iPSC-derived cardiac patch ReHeart/RiHeart
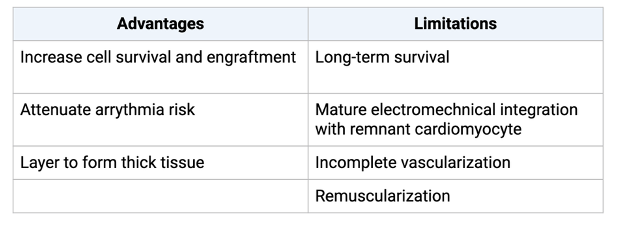
Unlike direct cell injection, cell sheets preserve cell-cell junctions and surface proteins to enhance cell survival and function5. These properties facilitate CM maturation and electrical coupling with host tissue, which may greatly reduce the risk of arrhythmia6. In addition, epicardial patch transplantation provides a less invasive and less damaging alternative to direct intramyocardial injection22,23. The sheet-based structure also improves cell survival and engraftment and can be layered to generate thicker tissues constructs for enhanced cell retention8,24. Moreover, the use of iPSC-CMs offers the potential for direct contractile
contribution and partial myocardial replacement25,26. Collectively, these advantages enabled ReHeart/RiHeart to successfully advance through clinical trials and become the first conditional approved iPSC-derived cardiac regenerative therapy in Japan3,4 (Table 1).
Nevertheless, several important limitations remain. Increased tissue thickness in multilayered cells sheets can lead to insufficient vascularization and reduced long-term cell survival24,27. Although sheet transplantation improves engraftment, the maturation of iPSC-CMs remains incomplete, resulting in immature electromechanical integration with host CMs28,29. Most importantly, definitive evidence demonstrating true long-term remuscularization of the injured myocardium is still lacking1,30. Overall, although significant challenges remain, the development of cardiac cell sheet technology and ReHeart/RiHeart represents a major milestone in translational cardiac regenerative medicine and provides a promising foundation for future strategies aimed at achieving true myocardial regeneration and functional heart repair4,31.
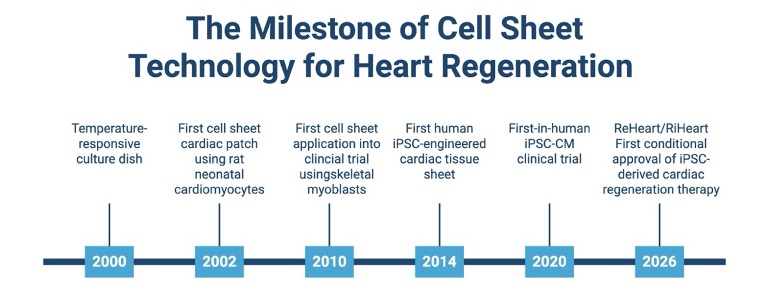
Figure 1. The milestone of cell sheet technology for heart regeneration. Created in BioRender. Cheng, Y. (2026) https://BioRender.com/1yhi233.
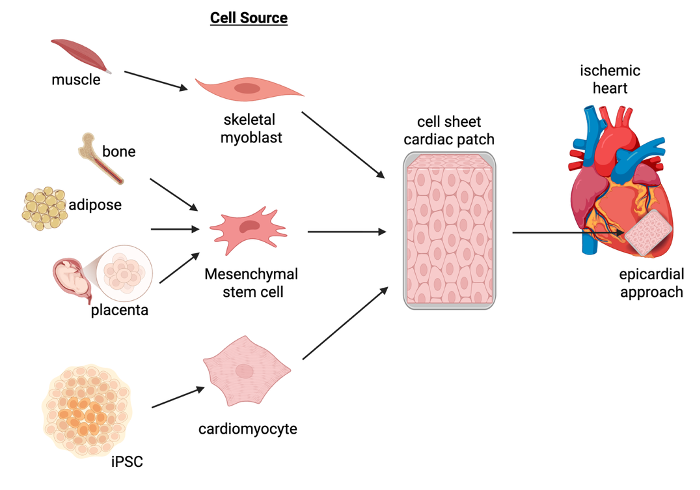
Figure 2. Various cell source to generate cell sheet cardiac patch for heart regeneration. Created in BioRender. Cheng, Y. (2026) https://BioRender.com/zuyt9z9.
Table 1. The advantages and limitations of ReHeart/RiHeart for cardiac regeneration. Created in BioRender. Cheng, Y. (2026) https://BioRender.com/2ixgd8m.
CONCLUSION
In this review, I summarized the historical development of cell sheet technology for cardiac regeneration and highlighted the major milestones that have driven progress in the field. The various cell sources were discussed to be used for generating cardiac cell sheets and the combination of iPSC technology with cell sheet engineering was presented as a promising strategy for heart regeneration. In addition, the major advantages and therapeutic potential of the current ReHeart/RiHeart platform were outlined, while the remaining limitations and challenges were addressed to be overcome to achieve true remuscularization and functional heart regeneration after injury. In conclusion, ReHeart/RiHeart represents a major step forward in translational cardiac regenerative medicine and provides an important foundation for the future development of clinically effective heart regeneration therapies.
ACKNOWLEDGEMENTS
This work was supported by grants from the National Science and Technology Council, Taiwan (NSTC 113-2311-B-038-005-MY2) and the National Health Research Institutes, Taiwan (NHRI-EX115-11424SC).
CONFLICT OF INTEREST
There is no conflict of interest.

Yuan-Yuan Cheng, Ph.D.
International Ph.D. Program in Cell College of Medicine, Taipei Medical University
Corresponding author:
112084@tmu.edu.tw
REFERENCES
- Eschenhagen T, Bolli R, Braun T, et al. Cardiomyocyte regeneration: a consensus statement. Nat Rev Cardial. 20117;14(9):563-579.
- Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126(4):663-676.
- Miyagawa S, Sawa Y. Building a new strategy for cardiac regeneration therapy using induced pluripotent stem cells. J Cardiol. 2018;72(6):445-448.
- Miyagawa S, Domae K, Yoshikawa Y, et al. Transplantation of human induced pluripotent stem cell-derived cardiomyocyte patches for ischemic cardiomyopathy. JACC Case Rep. 2022;4(7):396-400.
- Yang J, Yamato M, Nishida K, et al. Cell delivery in regenerative medicine: the cell sheet engineering approach. J Control Release. 2006;116(2):193-203.
- Zhang M, Methot D, Poppa V, Fujio Y, Walsh K, Murry CE. Cardiomyocyte grafting for cardiac repair: graft cell death and anti-death strategies. J Mol Cell Cardiol. 2001;33(5):907-921.
- Okano T, Yamada N, Sakai H, Sakurai Y. A novel recovery system for cultured cells using plasma-treated polystyrene dishes grafted with poly(N-isopropylacrylamide). J Biomed Mater Res. 1993;27(10):1243-1251.
- Shimizu T, Yamato M, Kikuchi A, Okano T. Cell sheet engineering for myocardial tissue reconstruction. Biomaterials.2003;24(13):2309-2316.
- Sawa Y, Miyagawa S, Sakaguchi T, et al. Tissue engineered myoblast sheets improved cardiac function sufficiently to discontinue LVAS in a patient with DCM: report of a case. Surg Today. 2012;42(2):181-184.
- Memon IA, Sawa Y, Fukushima N, et al. Repair of impaired myocardium by means of implantation of engineered autologous myoblast sheets. J Thorac Cardiovasc Surg. 2005;130(5):1333-1341.
- Miyahara Y, Nagaya N, Kataoka M, et al. Monolayered mesenchymal stem cells repair scarred myocardium after myocardial infarction. Nat Med. 2006;12(4):459-465.
- Masumoto H, Matsuo T, Yamamizu K, et al. Pluripotent stem cell-engineered cell sheets reestablish cardiac function in a rat myocardial infarction model. Circ Res. 2012;111(3):e8-e14.
- Menasché P. Skeletal myoblasts for cardiac repair. Expert Rev Cardiovasc Ther. 2005;3(1):21-27.
- Sekiya N, Matsumiya G, Miyagawa S, et al. Layered implantation of myoblast sheets attenuates adverse cardiac remodeling of the infarcted heart. J Thorac Cardiovasc Surg. 2009;138(4):985-993.
- Shudo Y, Miyagawa S, Fukushima S, et al. Novel regenerative therapy using cell sheet with omentopexy for damaged myocardium. J Thorac Cardiovasc Surg. 2013;145(5):1188-1196.
- Leobon B, Garcin I, Menasché P, et al. Myoblasts transplanted into rat infarcted myocardium are functionally isolated from their host. Proc Natl Acad Sci U S A. 2003;100(13):7808-7811.
- Gnecchi M, He H, Liang OD, et al. Paracrine action accounts for marked protection of ischemic heart by Akt-modified mesenchymal stem cells. Nat Med. 2005;11(4):367-368.
- Hamdi H, Planat-Bénard V, Bel A, et al. Epicardial adipose stem cell sheets result in greater post-infarction survival than intramyocardial injections. Cardiovasc Res. 2011;91(3):483-491.
- Murry CE, Soonpaa MH, Reinecke H, et al. Haematopoietic stem cells do not transdifferentiate into cardiac myocytes in myocardial infarcts. Nature. 2004;428(6983):664-668.
- Gnecchi M, Zhang Z, Ni A, Dzau VJ. Paracrine mechanisms in adult stem cell signaling and therapy. Circ Res.2008;103(11):1204-1219.
- Burridge PW, Keller G, Gold JD, Wu JC. Production of de novo cardiomyocytes: human pluripotent stem cell differentiation and direct reprogramming. Cell Stem Cell. 2012;10(1):16-28.
- Kawamura M, Miyagawa S, Fukushima S, et al. Enhanced survival of transplanted human induced pluripotent stem cell-derived cardiomyocytes by the combination of cell sheets with the pedicled omentum in a porcine heart. Circulation. 2013;128(11 Suppl 1):S87-S94.Haraguchi Y, Shimizu T, Yamato M, Okano T. Regenerative therapies using cell sheet-based tissue engineering for cardiac disease. Cardiol Res Pract. 2011:845170.
- Shimizu T, Yamato M, Isoi Y, et al. Fabrication of pulsatile cardiac tissue grafts using a novel 3-dimensional cell sheet manipulation technique and temperature-responsive cell culture surfaces. Circ Res. 2002;90(3):e40.
- Chong JJH, Yang X, Don CW, et al. Human embryonic-stem-cell-derived cardiomyocytes regenerate non-human primate hearts. Nature. 2014;510(7504):273-277.
- Laflamme MA, Murry CE. Heart regeneration. Nature. 2011;473(7347):326-335.
- Sekine H, Shimizu T, Yang J, Kobayashi E, Okano T. Pulsatile myocardial tubes fabricated with cell sheet engineering. Circulation. 2006;114(1 Suppl):I87-I93.
- Yang X, Pabon L, Murry CE. Engineering adolescence: maturation of human pluripotent stem cell-derived cardiomyocytes. Circ Res. 2014;114(3):511-523.
- Lundy SD, Zhu WZ, Regnier M, Laflamme MA. Structural and functional maturation of cardiomyocytes derived from human pluripotent stem cells. Stem Cells Dev. 2013;22(14):1991-2002.
- Laflamme MA, Murry CE. Heart regeneration. Nature. 2011;473(7347):326-335.\
- Matsuura K, Shimizu T. Cardiac cell sheet engineering for regenerative medicine and tissue modeling. Prog Mol Biol Transl Sci. 2023;197:127-154.

Leave a comment